The term “uvea” is derived from the Latin word “uva”, meaning “grape,” due to the resemblance of the choroidal lobules to a cluster of grapes. The suffix “-itis” means inflammation and is derived from Greek.
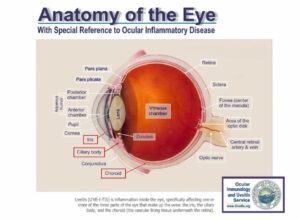
Uveitis is inflammation within the eye that primarily affects the uvea (the middle layer of the eye), which consists of three structures: the iris (the colored part of the eye), the ciliary body (located behind the iris and responsible for producing aqueous humor), and the choroid (the vascular layer beneath the retina). Problems associated with uveitis are relatively under-appreciated by the general population and ophthalmologists alike. Few people realize, for example, that uveitis is the fourth leading cause of blindness among the working-age population in this country.
Approximately sixty different conditions can cause uveitis, and the “detective work” involved in determining the underlying cause in a particular patient can be extremely tedious and costly. This “detective work” more closely resembles the diagnostic process in internal medicine than the typical practice of ophthalmology. Primarily for this reason, few ophthalmologists choose to specialize in uveitis.
Additionally, the care of some forms of uveitis requires the use of long-term systemic medications (nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and/or immunomodulatory therapy (IMT)). This also deters many ophthalmologists from managing patients with uveitis. However, there are several centers across the United States that specialize in the care of patients with uveitis, this potentially blinding condition. Additionally, increasing numbers of younger ophthalmologists are spending time, after completing their training in ophthalmology, getting specialty training so that they may care for patients with uveitis.
Both infectious, non-infectious, and malignant causes of uveitis are represented among patients seen at uveitis centers. Clearly, “getting to the bottom of it”—that is, definitively identifying the cause of the uveitis—is critical, as the choice of treatment depends heavily on the underlying etiology; a therapy appropriate for one cause may be harmful in patients with another.
Autoimmune noninfectious uveitis is the most common form of uveitis, and it tends to be recurrent. For uveitis treatment, we employ a stepladder approach to the management of patients with autoimmune uveitis. Treatment usually starts with topical corticosteroids and may escalate to injections or systemic therapy during the acute phase of disease. However, long-term treatment includes oral NSAIDs, conventional immunomodulatory therapy (IMT), biologic response modifier agents, small-molecule therapies, and, finally, cytotoxic agents. Our approach emphasizes limiting the total cumulative use of corticosteroids, given the high risk of potentially avoidable complications associated with prolonged, open-ended therapy. In addition, we maintain a strict intolerance for recurrent disease or persistent low-grade intraocular inflammation. This philosophy is grounded in over many years of research and clinical experience, which has demonstrated that allowing such recurrence or chronic low-grade inflammation leads to gradual but irreversible ocular damage and progressive vision loss.
We believe that as more physicians recognize the limited progress in reducing blindness due to uveitis, they will move away from traditional treatment approaches and adopt a zero-tolerance model for inflammation, using a stepwise treatment (stepladder) algorithm in managing patients with uveitis.
 |
|
|
|

Click on the Register link

In the email you receive, click on the change password link.

Change your password